
Question Is hypertension associated with the risk and severity of epistaxis?
Bạn đang xem: Association of Hypertension With the Risk and Severity of Epistaxis
Findings This nationwide population cohort study of 71 498 individuals found that, compared with patients without hypertension, those with hypertension appeared to have an increased risk of epistaxis, had more emergency department visits, and required more posterior nasal packing procedures.
Meaning This study suggests that hypertension is associated with an increased risk and severity of epistaxis.
Importance The association between hypertension and epistaxis has long been a subject of debate.
Objectives To evaluate the risk of epistaxis in patients with hypertension using a nationwide population cohort and to assess the association of hypertension with the methods of managing cases of epistaxis.
Design, Setting, and Participants In this retrospective cohort study, a hypertension cohort and comparison cohort were built using the Korean National Health Insurance Service-National Sample Cohort that represents the entire population of the Republic of Korea from January 1, 2002, to December 31, 2015. The hypertension cohort comprised 35 749 patients with a record of 3 or more prescriptions of antihypertensive medication and a diagnosis of hypertension (International Statistical Classification of Diseases and Related Health Problems, Tenth Revision code I10). Patients with other diseases associated with epistaxis, such as sinonasal tumors, facial trauma, bleeding tendency, and coagulation disorder, as well as those taking anticoagulant medications, were excluded. A comparison cohort comprised 35 749 individuals without hypertension matched sociodemographically in a 1:1 ratio. Statistical analysis was performed from January 1, 2019, to March 31, 2020.
Main Outcomes and Measures The incidence and recurrence of epistaxis were evaluated in both cohorts. The risk factors for epistaxis and management strategies were also assessed.
Results Among the 35 749 patients in the hypertension cohort (20 579 men [57.6%]; median age, 52 years [interquartile range, 45-62 years]) the incidence rate (IR) of epistaxis was 32.97 per 10 000 persons (95% CI, 30.57-35.51 per 10 000 persons); among the 35 749 individuals in the comparison cohort (20 910 men [58.5%]; median age, 52 years [interquartile range, 45-62 years]), the IR of epistaxis was 22.76 per 10 000 persons (95% CI, 20.78-24.89 per 10 000 persons) (IR ratio, 1.45; 95% CI, 1.29-1.63; adjusted hazard ratio, 1.47; 95% CI, 1.30-1.66). The IR of recurrent epistaxis was 1.96 per 10 000 persons in the hypertension cohort and 1.59 per 10 000 persons in the nonhypertension cohort (IR ratio, 1.23; 95% CI, 0.77-2.00). Patients with hypertension who experienced epistaxis were more likely to use the emergency department (odds ratio, 2.69; 95% CI, 1.70-4.25; Cohen h effect size, 0.27; 95% CI, 0.16-0.39) and receive posterior nasal packing (odds ratio, 4.58; 95% CI, 1.03-20.38; Cohen h effect size, 0.15; 95% CI, 0.03-0.26) compared with the comparison cohort.
Conclusions and Relevance This study suggests that patients with hypertension had an increased risk of epistaxis requiring hospital visits. In addition, epistaxis in patients with hypertension appeared to need more emergency department visits and require more posterior nasal packing procedures compared with patients without hypertension. Medical counseling about epistaxis is advisable for individuals with hypertension, and the presence of hypertension should be considered in managing nasal bleedings.
Epistaxis is a common condition and the leading cause of hospital visits.1 Although it is rarely life threatening, epistaxis is a cause of concern and requires appropriate treatment, especially in elderly patients with cardiovascular disease.1,2 Management strategies are variable depending on the severity of the bleeding. Minor hemorrhage can be relieved by simple compression or cauterization, but massive bleeding or recurrent bleeding with unidentified foci requires more invasive procedures, such as nasal packing, surgical ligation of vessels, or even endovascular management.1
Quiz Ref IDEpistaxis is thought to have multiple causes, such as dry air, infection, allergy, trauma, alcohol abuse, and the use of anticoagulants. Of the many risk factors, hypertension has been suggested as one of the more important conditions associated with the development of epistaxis, based on clinical impressions.3-6 Even though numerous studies have assessed the association between hypertension and epistaxis during the past decades,5,7-10 the association still remains unclear.7,8 In a recent systematic review and meta-analysis, hypertension was reported to be associated with a significantly increased risk of epistaxis in case-control studies.8 Some previous studies, however, reported that there was no meaningful association between epistaxis and hypertension.10-12
To answer the question whether hypertension is a risk factor for epistaxis or a physiologic response to nasal bleeding followed by adrenergic effect and anxiety, we planned a nationwide population-based study. The aim of this study was to evaluate the risk of epistaxis for patients with hypertension using a nationwide cohort. Patients with other known risk factors for nasal bleeding were excluded from the cohort to minimize possible bias in interpreting the results. A comparison cohort consisted of patients without hypertension who were carefully matched on sociodemographic factors and comorbidity index. In addition, hospital visits and methods of management of epistaxis were evaluated to evaluate the association of hypertension with the severity of epistaxis.
The National Health Insurance Service-National Sample Cohort is a population-based cohort constructed by the Korean National Health Insurance Service (KNHIS). A sample cohort was established January 1, 2002, by systematic stratified random sampling, to represent the entire population (50 million) registered in South Korea. The cohort comprises 2.2% of the total Korean population (1 million) and was followed up for 13 years until December 31, 2015. The cohort database includes (1) personal information, (2) diagnostic codes, (3) procedures and prescription codes, (4) socioeconomic information (residence and income), (5) records of medical service use, and (6) death records. After data selection, the relevance of the sample cohort was verified by comparing data from the entire Korean population and from the sample cohort. Details of the methods used have been provided by the KNHIS (http://nhiss.nhis.or.kr/). This investigation was approved by the local ethics review board (Hanyang University Guri Hospital Institutional Review Board) and was performed in accordance with the Declaration of Helsinki13 and good clinical practice guidelines. As the study used deidentified data from the KNHIS sample cohort, patient consent was waived by the Hanyang University Guri Hospital Institutional Review Board.
Permission was obtained to use the KNHIS sample cohort database for medical information in this study. The diagnostic classifications followed the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10). We declare no conflicts of interest with the NHIS.
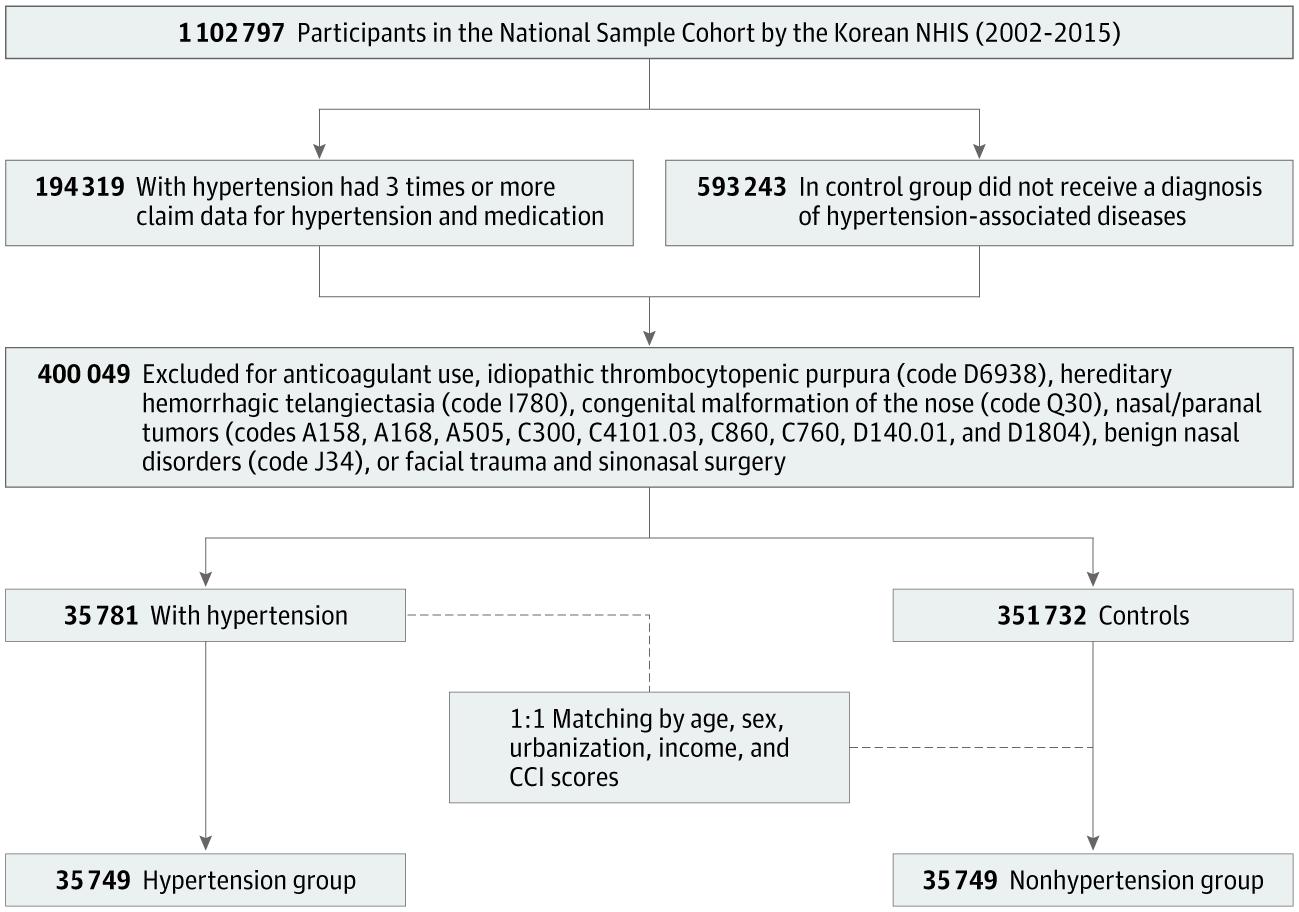
A total of 194 319 patients who met the inclusion criteria (a record of 3 or more claims for prescriptions of antihypertensive medication with a diagnosis of hypertension) since 2002 were selected (Figure). Patients with other risk factors for nasal bleeding, such as sinonasal tumor, facial trauma, rhinologic surgery, bleeding tendency, and coagulation disorder, as well as those taking anticoagulant medications (heparin, enoxaparin, abciximab, warfarin, clopidogrel, ticlopidine, and low-dose aspirin), were excluded. Patients with hypertension were matched 1:1 with individuals who had never received a diagnosis of hypertension from 2002 through 2015 (Figure). Matching was performed for age, sex, income, dwelling place, and the Charlson Comorbidity Index (CCI) score. The hypertension cohort and the comparison cohort included 35 749 individuals each.
To prevent selection bias when selecting the matched participants, the comparison participants were sorted using random numbers and then were selected in order. It was assumed that the matched control participants were recruited at the same time as the patients with hypertension were enrolled. After propensity score matching, the occurrence of epistaxis was followed up from the enrolled time point to 2015. Charlson Comorbidity Index scores comprising 17 medical comorbidities (eg, congestive heart failure, dementia, diabetes, and liver disease) were calculated from 0 to 33 (where higher scores indicate more comorbidities) using the previously validated algorithm based on ICD-10 data.14
Xem thêm : 10 things that you can add to your water while fasting!
Patients with hypertension were defined as those with the diagnostic codes of essential hypertension (ICD-10 codes I10, I10.0, I10.1, and I10.9) who used medical services 3 times or more and received antihypertensive medications. Patients with epistaxis were defined as those with the diagnostic code of epistaxis (ICD-10 code R04.0). Recurrence of epistaxis was defined as a repeated episode more than 90 days after the treatment of epistaxis. Patients with a diagnosis of other hemorrhagic disorders or sinonasal tumorous conditions—idiopathic thrombocytopenic purpura (ICD-10 code D6938), hereditary hemorrhagic telangiectasia (ICD-10 code I780), congenital malformation of the nose (ICD-10 code Q30), nasal or paranal tumors (ICD-10 codes A158, A168, A505, C300, C4101.03, C860, C760, D140.01, and D1804), and benign nasal disorders (ICD-10 code J34)—at any point during the study period were excluded from the analysis. Patients with posttraumatic or iatrogenic epistaxis were also excluded, such as those who experienced epistaxis within 30 days of head trauma (ICD-10 codes S00-S09) or nasal surgery. Epistaxis management was assessed by reviewing the procedure codes of cauterization, anterior nasal packing, posterior nasal packing, arterial ligation, septoplasty, or endoscopic sinus operations.
Statistical analysis was performed from January 1, 2019, to March 31, 2020. Data were analyzed with the use of SAS Enterprise Guide software, version 7.1 (SAS Institute Inc). Propensity score matching was used to reduce selection bias between the hypertension and comparison groups, and propensity scores were calculated based on age, sex, urbanization, income, and CCI score. The demographic characteristics of the study population are presented as percentages for categorical variables and mean (SD) values for continuous variables. The standardized difference was identified to assess the balance of covariates after matching. Incidence rates per 10 000 person-years were calculated with 95% CIs. Incidence rate ratios for epistaxis occurrence and recurrence were calculated in the hypertension cohort relative to the comparison group. A Cox proportional hazards regression model was used to analyze the risk of epistaxis (hazard ratio). A comparison of management methods was performed using χ2 tests. Odds ratios (ORs) and Cohen h effect sizes were also calculated.
This study used the KNHIS sample cohort database with permission. Data can be shared by request from any qualified investigator for purposes of replicating procedures and results.
During the study period, a total of 194 319 adult patients received antihypertensive medication and visited clinics 3 or more times with a diagnosis of hypertension. By excluding diseases associated with epistaxis, 35 781 patients with hypertension were matched 1:1 with the comparison group without hypertension for age, sex, socioeconomic status, and CCI score (Figure).
Among the 35 749 patients in the hypertension cohort, 20 579 were men (57.6%), and the median age was 52 years (interquartile range [IQR], 45-62 years); among the 35 749 individuals in the comparison cohort, 20 910 were men (58.5%), and the median age was 52 years (IQR, 45-62 years) (Table 1). The median follow-up period was 5.5 years (IQR, 2.8-8.9 years) in the hypertension group and 5.6 years (IQR, 2.9-9.0 years) in the comparison group.
In the hypertension group, 696 patients visited hospitals complaining of epistaxis during the observation period, while 483 individuals in the nonhypertension group developed epistaxis (Table 1). Quiz Ref IDThe overall incidence rate of epistaxis in the hypertension group was 32.97 per 10 000 persons (95% CI, 30.57-35.51 per 10 000 persons), 1.45 (95% CI, 1.29-1.63) times higher than in the nonhypertension group (22.76 per 10 000 persons; 95% CI, 20.78-24.89 per 10 000 persons) (Table 2).
In multivariable analysis of the whole cohort, the presence of hypertension was a significant risk factor for the development of epistaxis (crude hazard ratio, 1.47; 95% CI, 1.30-1.65; adjusted hazard ratio, 1.47; 95% CI, 1.30-1.66). Other considered factors (including age, sex, CCI score, income, and urbanization level) were not significant.
Recurrent epistaxis was identified in 42 of 696 patients in the hypertension group and 34 of 483 patients in the nonhypertension group (Table 1). The incidence rate of recurrent epistaxis was 1.96 per 10 000 persons in the hypertension group (95% CI, 1.41-2.65 per 10 000 persons) and 1.59 per 10 000 persons (95% CI, 1.10-2.22 per 10 000 persons) in the nonhypertension group (Table 3). The incidence rate ratio of epistaxis recurrence was 1.23 (95% CI, 0.77-2.00), which did not show clinically meaningful differences.
A total of 89 of 696 patients with hypertension (12.8%) visited the emergency department for epistaxis, as did 25 of 483 patients without hypertension (5.2%) (OR, 2.69; 95% CI, 1.70-4.25; Cohen h effect size, 0.27; 95% CI, 0.16-0.39) (Table 4). Patients in the nonhypertension group visited primary care clinics more frequently than did patients in the hypertension group (OR, 0.55; 95% CI, 0.40-0.75; Cohen h effect size, −0.23; 95% CI, −0.35 to −0.12).
A total of 524 of 696 patients with hypertension (75.3%) and 392 of 483 patients without hypertension (81.2%) were managed with noninvasive methods, including topical vasoconstriction and simple cauterization (Table 4). Quiz Ref IDPatients with hypertension needed more posterior nasal packing procedures compared with those in the nonhypertension group (13 of 696 [1.9%] vs 2 of 483 [0.4%]) (OR, 4.58; 95% CI, 1.03-20.38; Cohen h effect size, 0.15; 95% CI, 0.03-0.26) (Table 4).
This study used nationwide medical data to evaluate whether hypertension is a possible risk factor for epistaxis. Patients with hypertension had a 1.47 times higher risk of epistaxis than individuals without hypertension (adjusted hazard ratio, 1.47; 95% CI, 1.30-1.66). There was no meaningful difference in the risk for recurrent epistaxis between the hypertension and nonhypertension groups (incidence rate ratio, 1.23; 95% CI, 0.77-2.00). Patients with hypertension who experienced epistaxis appeared to use the emergency department more often (OR, 2.69; 95% CI, 1.70-4.25; Cohen h effect size, 0.27; 95% CI, 0.16-0.39) and require more posterior nasal packing procedures (OR, 4.58; 95% CI, 1.03-20.38; Cohen h effect size, 0.15; 95% CI, 0.03-0.26) than did patients without hypertension. To our knowledge, the present study is the first to assess the association between hypertension and epistaxis using a nationwide population-based cohort. The results suggest that hypertension may be a risk factor for epistaxis.
The association between hypertension and epistaxis has been a longstanding debate. Even though there have been numerous studies on the subject during the past decades, it still remains controversial whether hypertension is a risk factor for epistaxis or a physiologic response to nasal bleeding followed by an adrenergic effect.8,15 In this study, the hypertension cohort and nonhypertension comparison cohort were constructed to evaluate the longitudinal association of hypertension with the occurrence of epistaxis (Figure). Patients with other possible risk factors for epistaxis were excluded, and a comparison cohort was carefully matched on sociodemographic factors and CCI score (Table 1). The result showed that patients with hypertension appeared to have more episodes of epistaxis requiring hospital visits than did patients without hypertension, with a higher incidence and severity of epistaxis. The recurrence of epistaxis was not significantly different between the hypertension cohort and comparison cohort (Table 3). Quiz Ref IDThis result was compatible with a previous report suggesting that risk factors for recurrent epistaxis were unidentified bleeding points, the treatment strategy used in the initial bleeding episode, and posterior nasal bleeding, rather than clinical characteristics or comorbidities.6 It is still theoretically possible, however, that recurrence of epistaxis may be higher for patients with hypertension, which could not be assessed in this study owing to the limitation of public claims data.
The present study evaluated the severity of epistaxis indirectly by assessing the hospital visits and management strategies used. Regarding the severity of epistaxis, this study showed that patients with hypertension were more likely to visit the emergency department for epistaxsis and be managed by posterior nasal packing compared with the cohort without hypertension (Table 4). The results are compatible with the widely accepted sense that nasal bleeding in patients with hypertension is more difficult to control, which clinicians should be aware of when managing nasal bleeding.
Among approximately 60% of the general population of people who would experience episodes of epistaxis in their lifetime,1 it was reported that 6% need medical or surgical management and that less than 0.2% require hospitalization for bleeding control.7 In our study, the incidence rate of epistaxis that required a hospital visit was 32.97 per 10 000 persons in the hypertension cohort and 22.76 per 10 000 persons in the nonhypertension cohort (Table 2). In the United States, a review of 57 039 patients who were hospitalized with epistaxis showed that 38.3% were treated conservatively, 53.3% received nasal packing or cauterization, 4.7% underwent arterial ligation, and 3.4% underwent embolization.1 Although the present study yielded a similar pattern of epistaxis management, there was a smaller proportion of patients who received surgical management than in the US study. This difference was probably due to the exclusion in the present study of individuals with possible comorbidities of serious epistaxis, such as nasal tumor or hemorrhagic conditions. Moreover, the higher primary accessibility of otolaryngologists and nasal endoscopes in South Korea may also have influenced the current results.
Chronic vascular damage has been suggested as a possible pathophysiological mechanism by which hypertension is associated with epistaxis. In a postmortem study, degenerative fibrous changes of nasal vessels were observed in patients with hypertension.16 Arterial hypertension could damage the vascular endothelial wall via oxidative stress.17 Various histologic changes to the vascular wall due to hypertension were known to result in the formation of atherosclerotic plaques, which render vessels fragile.5 Patients with hypertension experiencing epistaxis showed a higher prevalence of retinal artery atherosclerosis, which is often referred to as a “window” to vascular health,18 and patients with hypertensive retinopathy had more frequent episodes of epistaxis.2
The medical insurance system in South Korea was first implemented in 1977 and then expanded to cover the entire registered Korean population in 1989. The NHIS of Korea is a single-payer system, and data related to medical care are maintained in the NHIS database. The present study used the representative sample cohort, which has statistical strength and reflects the entire nation. Because the NHIS cohort data contain only diagnostic codes, procedures performed, and medication prescribed, detailed clinical information (such as severity of hypertension, patient adherence, specific bleeding foci, amount of bleeding, or evaluation of successful management) could not be assessed. In addition, patients with mild episodes of epistaxis who did not visit clinics could not be evaluated in this study using the NHIS claims data. Although it is not possible to show that all cases of epistaxis occurred more often in patients with hypertension, we can still conclude that nasal bleeding that required hospital visits and needed more advanced management methods was more prevalent in patients with hypertension. In the future, the issues raised about the severity of both epistaxis and hypertension and their association with each other will need to be addressed,19 as well as whether the successful management of hypertension can reduce the incidence and severity of epistaxis.
This study has some strengths. To investigate the question whether epistaxis is associated with hypertension, the present study tried to build a nationwide population cohort. To minimize biases, patients with possible confounding risk factors for epistaxis were excluded, and the comparison cohort was matched with the hypertension cohort on socioeconomic factors and CCI scores. We also indirectly assessed the severity of hypertension by reviewing the pattern of hospital visits and the management strategies for epistaxis.
Xem thêm : How to Say Food in Spanish? A Quick Guide to Foods in Spanish
This study also had some limitations, mostly stemming from the characteristics of the claims data research, because they do not include physical examination data (such as systolic and diastolic blood pressure and specific bleeding focus or the amount of epistaxis). Quiz Ref IDIn addition, owing to the strict operational definition of hypertension to avoid selection errors, the hypertension group could not include patients with poor adherence who did not visit clinics regularly and who might have had more complications.
This nationwide population cohort study found that patients with hypertension appeared to have an increased risk of epistaxis requiring hospital visits. In addition, patients with epistaxis and hypertension appeared to need more emergency department visits and required more posterior nasal packing procedures than did patients with epistaxis without hypertension. Medical counseling about epistaxis is advisable for individuals with hypertension, and the presence of hypertension should be considered when managing nasal bleeding.
Accepted for Publication: July 20, 2020.
Published Online: September 10, 2020. doi:10.1001/jamaoto.2020.2906
Correction: This article was corrected on December 10, 2020, to fix an error in the Figure.
Corresponding Author: Jae Ho Chung, MD, PhD, Department of Otolaryngology-Head and Neck Surgery, School of Medicine, Hanyang University, 222-Wangshimni-ro, Seongdong-gu, Seoul, 04763, Korea (jaeho.chung.md@gmail.com).
Author Contributions: Dr Byun and Ms Ryu had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Chung, Lee, Kim, Shin.
Acquisition, analysis, or interpretation of data: Byun, Chung, Ryu.
Drafting of the manuscript: Byun, Chung, Lee.
Critical revision of the manuscript for important intellectual content: Byun, Chung, Ryu, Kim, Shin.
Statistical analysis: Chung, Ryu, Shin.
Obtained funding: Chung.
Administrative, technical, or material support: Byun, Chung, Shin.
Supervision: Chung, Lee, Kim.
Conflict of Interest Disclosures: None reported.
Funding/Support: This research was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education (NRF-2017R1D1A1B03033051).
Role of the Funder/Sponsor: The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Nguồn: https://blogtinhoc.edu.vn
Danh mục: Info
This post was last modified on Tháng mười một 25, 2024 4:24 chiều